The Assembly
In the beginning, there is only scattering—
a thousand fragments on white cloth,
no map to guide the searching fingers,
no promise that completion lives
within this chaos.
First, the corner pieces arrive like prophecies:
crystalline with potential,
their edges sharp as morning light.
They sing of how the world might fit—
these architects of hope,
these blueprints drawn in possibility,
luminous with the logic of what could be.
Then come the measured ones,
born in sterile chambers
where variables bow to control.
Perfect in their small dominions,
they lock together with mathematical certainty—
until you carry them beyond their borders
and find they speak a foreign tongue
to the wild grammar of living,
their clean lines fracturing
against the beautiful chaos of skin and breath.
Here too, the heirloom pieces,
worn silk-smooth by countless hands
that searched this same impossible picture.
They hold the weight of accumulated wisdom,
each curve a whispered story,
each surface polished by the faith
of those who came before,
their edges gentled by the patient work
of masters who have seen
ten thousand puzzles bloom.
And the field-tested fragments—
scarred by weather,
marked by the honest friction
of theory meeting flesh,
of hope encountering the daily grind
of hearts still ticking in the fluorescent hush
of waiting rooms,
these pieces that know the difference
between what works on paper
and what holds when the world
presses its full weight
against your careful plans.
Last arrive the pieces you must enter,
not merely place—
the ones that demand you live inside them,
where abstract becomes breath,
where possibility becomes the morning
you wake up and whisper
to the startled air:
I am not who I was yesterday.
Here, the picture is no longer something
you assemble
but something that assembles you.
Truth is the moment when all languages
suddenly speak as one—
when the theoretical corner
embraces the lived center,
when ancient wisdom holds hands
with the breathing moment,
when what should be
kisses what is
and neither is diminished,
when all the scattered pieces
find their true names
in the country of your healing.
We are all apprentices here,
learning which edges hunger for each other,
which gaps are not failures
but windows,
which broken places
are invitations
to imagine new geometries of wholeness.
Some puzzles will never complete—
and this too is wisdom:
knowing when to honor the scattered,
when to begin again with grace,
when to trust that the picture we need
exists just beyond
the borders of what we can see,
waiting for us to grow
large enough to hold it.
Introduction: The Question That Started Everything
"How do we actually know what works?"
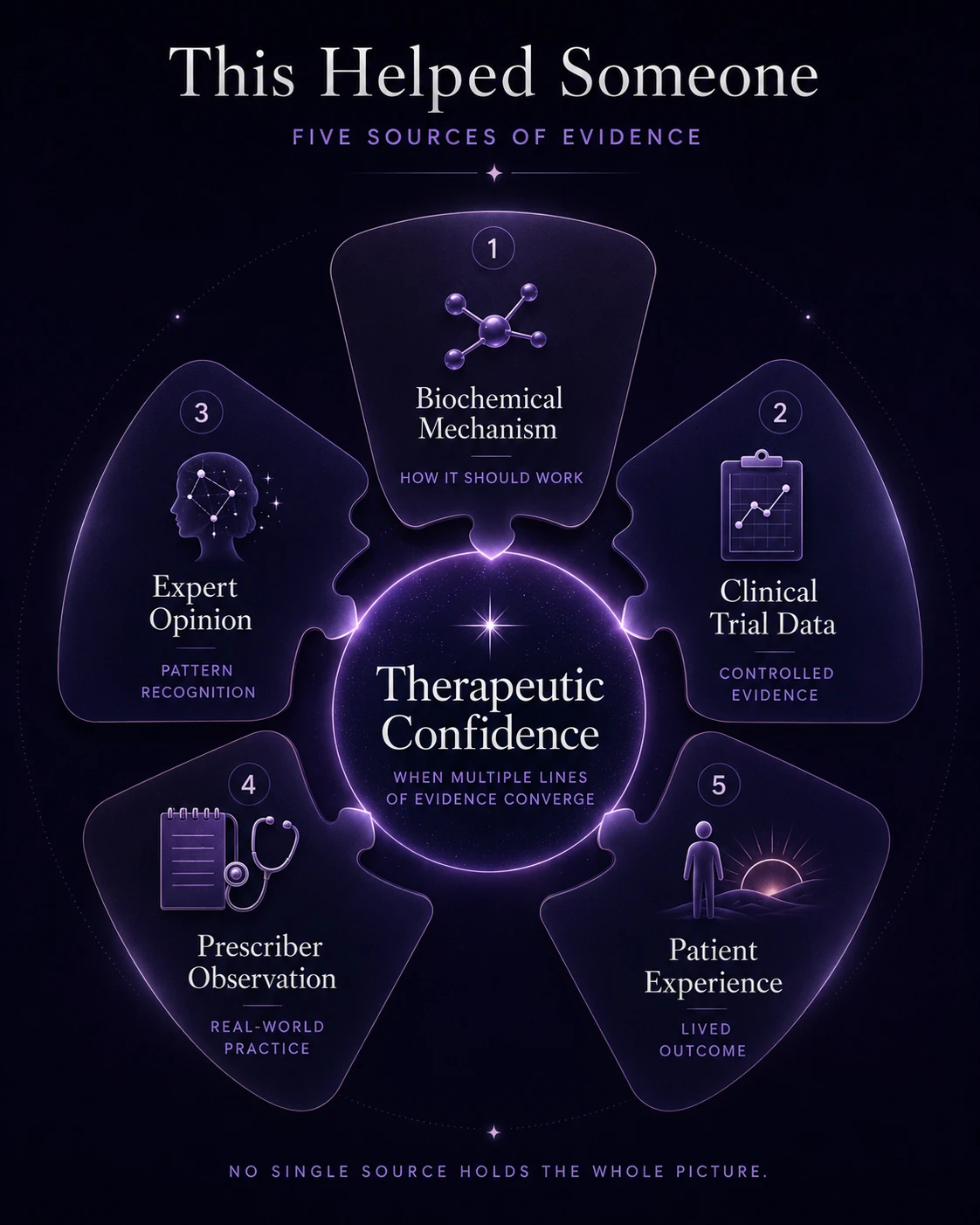
Truth in psychiatric medicine doesn't emerge from any single source. It emerges when multiple ways of knowing converge—like pieces of a puzzle finally fitting together. This convergence reveals something profound: psychiatric medicine has less of a knowledge problem than a knowledge integration problem.
The biochemist understands receptor binding but misses lived experience. The clinical investigator captures statistical significance but loses individual variation. Prescribers can capture complex real-world outcomes over time but may experience confirmation bias or selection bias. The expert has seen so many cases they may be able to recognize rare patterns, but they may be resistant to paradigm shifts. The patient knows their own experience but lacks the broader context.
Each holds essential pieces. None holds the complete picture.
This document describes a practical framework for evaluating what works in psychiatric treatment. It's meant for anyone navigating this complex terrain—patients, prescribers, families, and researchers. The framework shows how to examine evidence from multiple angles, recognizing when different types of truth align to create what I call "therapeutic confidence"—and equally important, when they don't.
The pages that follow explore this integration challenge through both conceptual models and lived experience, offering tools to navigate the space between theory and practice, between hope and evidence.
The Framework: How We Know What Works
Finding effective treatment is like assembling a puzzle where each piece represents a different type of evidence. When we understand what each piece can and cannot tell us, we begin to see how therapeutic truth emerges.
The Five Sources of Evidence
The Philosophical Foundation: Why No Single Source Holds Truth
Before examining each evidence source, we must address a fundamental question: How do we know what we know in psychiatry?
Traditional medicine often seeks foundational truth—a bedrock fact from which all other knowledge flows. Find the pathogen, identify the lesion, isolate the deficiency. This is foundationalist epistemology: truth built on unshakeable ground. It works beautifully for strep throat or broken bones.
But consciousness resists this approach. There is no blood test for suffering, no brain scan for hope, no assay that captures what it feels like when the darkness lifts. Psychiatric truth isn't foundational—it's coherentist. Truth emerges not from any single authoritative source, but from the convergence of multiple independent lines of evidence that support and validate each other.
Consider a mechanistic study which shows:
Molecular (days): Acute SERT occupancy in dorsal raphe → transient 5‑HT1A autoreceptor hyperstimulation → reduced raphe firing; predicted time course of autoreceptor desensitization (≈10–21 days) restoring tonic and phasic output; secondary 5‑HT1B heteroreceptor effects at cortical/striatal terminals. Cellular (weeks): ↑ BDNF/TrkB signaling, mTOR/eEF2 shifts, AMPAR insertion, spine density changes in mPFC/hippocampus; predicted direction and latency of plasticity markers. Circuit (weeks): Normalization of sgACC–DMN hyperconnectivity; enhanced fronto‑striatal reward throughput (ventral striatum/VTA phasic bursting). Prediction: reduced pathological self‑referential loops; improved reward responsiveness. Systems/behavior (weeks): On the Probabilistic Reward Task, increased response bias to high‑value cues; effort‑discounting shifts toward higher effort for reward; attention‑bias moves away from loss/rumination stimuli. Biomarkers (anchors, not arbiters): qEEG frontal alpha asymmetry drifts toward euthymic norms; task‑based striatal BOLD ↑ to reward; serum BDNF modest ↑; inflammatory panel (CRP/IL‑6) trends ↓ in responders; kynurenine/tryptophan ratio shifts toward anti‑inflammatory profile. Contrasts to distinguish mechanisms: If benefit is sedation‑mediated, expect no improvement on reward‑learning tasks and a distinct qEEG signature; if reward‑circuit driven, predict the opposite pattern.
We then ask: do trials, prescribers, and patients show changes that cohere with these predictions, on the timetable the model proposes? If several layers align—and the mismatches have plausible, testable explanations—we raise confidence. If they don’t, we revise the model. Coherence across levels, not a single slogan, earns belief.
This isn't relativism—not all perspectives are equal. It's recognition that psychiatric truth is irreducibly complex, requiring multiple viewpoints to triangulate reality. Like sudoku where each number is constrained by rows, columns, and boxes simultaneously, psychiatric evidence gains validity through multiple constraints aligning.
This philosophical commitment shapes everything that follows. We're not searching for the "real" truth beneath all others. We're mapping how different truths relate, reinforce, or contradict each other. When mechanism contradicts experience, we don't dismiss experience as "anecdotal." When trials contradict clinical practice, we don't assume practice is wrong. We investigate why these truths diverge and what that divergence teaches us.
1. Biochemical Mechanism (Corner Pieces): How a drug should work based on brain chemistry—receptor targets, neurotransmitter effects, and metabolic pathways. These corner pieces orient the entire picture but reveal little of the actual image.
What it tells us: Causal logic, biological plausibility, side effect prediction. What it misses: Human complexity often makes elegant theories crumble. Example: Multiple SSRIs with similar mechanisms producing vastly different responses in the same person.
2. Clinical Trial Data (Numbered Sections): Statistical proof of efficacy in controlled conditions, usually compared to a placebo. These pieces fit together perfectly within their controlled environment but may not connect elsewhere.
What it tells us: Quantifiable outcomes under standardized conditions. What it misses: Real-world complexity—comorbidities, polypharmacy, individual variation. Example: Trials showing SSRI efficacy while real patients repeatedly retry the same medications hoping for renewed efficacy, only to find diminishing returns.
3. Expert Opinion (Master Assemblers): Pattern recognition from specialists who've seen thousands of patients over years of practice. They know which patterns typically work but may miss novel configurations.
What it tells us: Nuanced synthesis of multiple sources, rare event identification. What it misses: Can become dogmatic and resistant to paradigm shifts. Example: Believing that while older medications may have more evidence of success, new medications cannot also be effective.
4. Prescriber Observation (Field Testing): How medications perform in day-to-day practice with diverse patients. This real-time assembly reveals which theoretical connections actually hold under pressure.
What it tells us: Real-world effectiveness, long-term outcomes, unexpected uses. What it misses: Selection bias, confirmation bias, limited sample sizes. Example: A practitioner may see stimulants producing "improvement" in productivity without recognizing that some patients are merely becoming more efficient at dysfunctional patterns—more content with their limitations rather than addressing underlying issues.
5. Patient Experience (The Living Result): The ultimate outcome: does life actually improve? This is the completed picture that patients must inhabit, serving as the final validation of all prior assembly work.
What it tells us: Functional improvement, quality of life, meaningful change. What it misses: Can be misleading with certain drug classes, attribution errors. Example: Feeling "stimulated" and more functional while remaining fundamentally unchanged.
The Key Insight: When all five sources align, we achieve therapeutic confidence—not because we've found foundational truth, but because independent lines of evidence have converged toward the same conclusion. This coherence, not any single authority, is what makes psychiatric knowledge reliable. When they conflict, critical investigation is needed. When none fit, we might be working with entirely the wrong puzzle.
Assembling the Picture: Convergence, Confidence, and Humility
The fundamental challenge in psychiatric medicine isn't gathering information—it's knowing how to trust it. How do we move from scattered evidence to therapeutic confidence?
When Truth Emerges
Therapeutic confidence crystallizes through convergence—when mechanism predicts what trials suggest, trials reflect what experts expect, experts anticipate what practitioners observe, and practitioners see what patients experience. This alignment creates not certainty, but a reasonable belief grounded in multiple forms of evidence. It's the quiet moment when possibility flows into probability, when inherited wisdom embraces lived experience.
When Single Sources Mislead
Each type of evidence, considered alone, can profoundly mislead:
The Mechanism-Expert Trap: An expert's prescriber's guide once claimed MAOIs require no tapering because they "self-taper" through irreversible enzyme inhibition. This is theoretically elegant, but a prescriber who has prescribed these medications enough, or a patient who has taken them, knows they need to be gradually tapered.
The Trial Distortion: How do you double-blind psychedelic research? Who volunteers for such studies? Often, it's people displaying more openness, a willingness to cede control, and those already comfortable with consciousness exploration. This can create a selection bias before the first dose is administered.
The Experience Paradox: Stimulants can make most people feel more productive and engaged. But even with extended-release formulations, many patients remain intensely aware the effects will wear off soon, leaving them depressed again. The subjective experience of "improvement" can mask a fundamental dysfunction, making someone more content with it rather than resolving it. This is precisely why single-source evidence misleads—only through convergence can we distinguish genuine therapeutic benefit from mere symptom suppression. Without integrating multiple perspectives, we risk mistaking transient relief for genuine therapeutic progress.
This is why convergence matters: it protects us from the seductive simplicity of single-source certainty.
The Multi-Axial Framework: A Visual Guide to Sources of Truth
EVIDENCE SOURCE
STRENGTHS
LIMITATIONS
TRUTH TYPE
Mechanistic Theory
Provides causal logic
Predicts side effects
Guides combinations
Often reductionist
May oversimplify complexity
Theory ≠ reality
Possible truth
Controlled Trials
Statistical rigor
Standardized variables
Quantifiable outcomes
Artificial conditions
Limited generalizability
Excludes complex patients
Statistical truth
Expert Synthesis
Pattern recognition
Integrates multiple sources
Captures nuance
Authority bias
Can resist paradigm shifts
Limited by experience
Interpreted truth
Prescriber Observation
Real-world effectiveness
Captures complexity
Long-term outcomes
Confirmation bias
Anecdotal nature
Selection effects
Practical truth
Patient Experience
Ultimate functional outcome
Quality of life
Person-centered focus
Highly subjective
Individual variation
Attribution errors
Lived truth
Having established how we evaluate evidence through multiple sources, we now turn to another dimension of understanding: the different levels at which medications operate. Each level provides a distinct lens for comprehending therapeutic effects.
Levels of Understanding: Three Ways to View Medication Effects
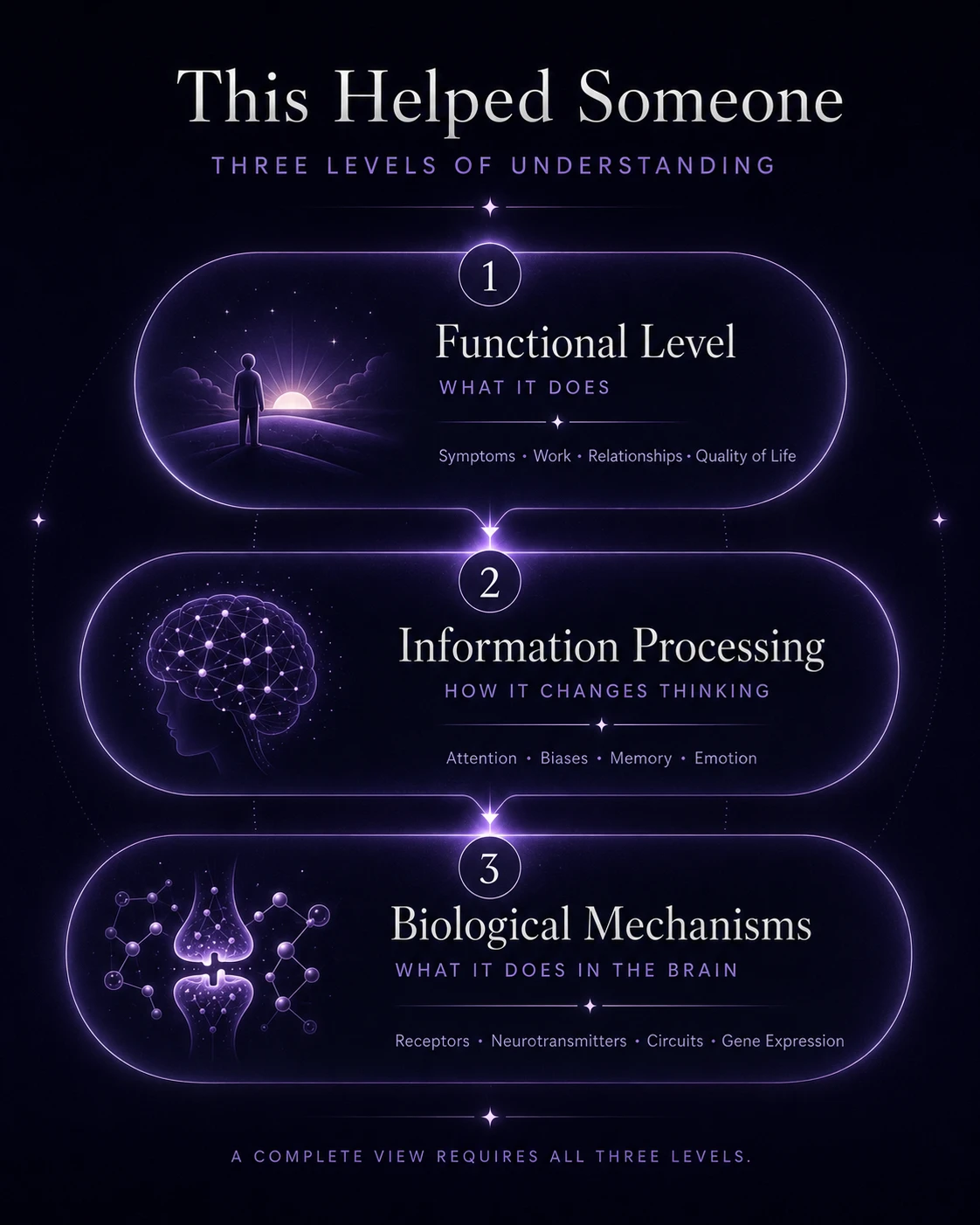
Beyond examining how we know medications work, we must consider the different levels at which they operate. Each level provides a distinct lens, and all three are necessary for a comprehensive understanding.
The Three Levels
1. FUNCTIONAL LEVEL
"What it does"
Reduces symptoms Enables work Improves relationships Restores quality of life
2. INFORMATION PROCESSING
"How it changes thinking"
Alters attention Shifts cognitive biases Modifies memory formation Changes emotional processing
3. BIOLOGICAL MECHANISMS
"What it does in the brain"
Binds to receptors Modifies circuits Alters neurotransmitters Changes gene expression
The Functional Level addresses the ultimate question: Does this medication help someone live the life they want to live? It focuses on observable outcomes like reduced symptoms, improved relationships, and a return to meaningful activity.
The Information Processing Level examines how medications alter mental algorithms, such as reducing rumination, enhancing cognitive flexibility, and modifying emotional processing priorities.
The Biological Level reveals the physical implementation: receptor activation, neurotransmitter modification, and circuit reorganization.
Choosing Your Starting Point
In our Discord community, there's a tendency to obsess over biological detail. Often, this isn't the most helpful starting point. If we knew every intricate detail about the brain and how drugs affect neural networks, this might be sufficient, but since that knowledge remains incomplete, the patterns are less clear.
Starting with function is often more useful because behaviors are measurable. When a patient finds effective treatment, the functional changes are often undeniable: they can date again, apply for jobs, and enjoy social interaction. Combining functional observation with information processing insights reveals what drugs actually accomplish.
Consider this: psychedelics like psilocybin have vastly different mechanisms from dissociatives like ketamine on a molecular level. Yet both can evoke rapid changes in thought patterns and lead to swift behavioral transformation. Perhaps success comes not from mechanistic similarity, but from functional equivalence.
Real-World Application: Three Medications That Work
Here is a demonstration of how this framework applies to three particularly effective antidepressants, showing how converging evidence builds therapeutic confidence.
For Anhedonic Depression: Tranylcypromine (Parnate)
When depression features profound anhedonia, avolition, and energy depletion.
Mechanism: Irreversible MAO‑A/B inhibition → sustained ↑ synaptic NE/DA; concomitant ↑ trace amines (e.g., PEA) with TAAR1 modulation of monoaminergic firing patterns. Predictions: greater phasic dopamine signaling in mesolimbic pathways (motivation/effort valuation), improved initiation/energy in anhedonic profiles; on tasks, ↑ willingness to exert effort for reward; on qEEG, beta‑band changes consistent with arousal/motivation rather than sedation. Trials: Limited modern data, but existing studies often show efficacy in treatment-resistant cases where anhedonia dominates. Expert Opinion: Specialists in treatment-resistant depression have realized their value over a long period of time and a very large number of cases. Prescriber Observation: Practitioners experienced with MAOIs note their utility in patients needing dopaminergic activation, though such prescribers remain scarce. Patient Experience: Highly rated and praised.
Result: Multiple sources pointing toward dopaminergic intervention → High confidence for anhedonic depression.
For Anxious Depression: Phenelzine (Nardil)
When depression interweaves with significant anxiety or social phobia.
Mechanism: Irreversible MAO‑A/B inhibition plus inhibition of GABA‑transaminase via the PEH metabolite → modest ↑ cortical GABA alongside monoamine increases. Predictions: stronger anxiolysis (GABA) with antidepressant effect (monoamines); behaviorally, ↓ autonomic reactivity and anticipatory anxiety; physiologically, improved sleep continuity and lower startle. Trials: Historical efficacy in "atypical depression" and social anxiety disorder. Expert Opinion: Those familiar with MAOIs note phenelzine's particular efficacy for anxiety-prominent presentations. Prescriber Observation: Often reserved for treatment-resistant depression with anxiety components, with observed anxiolytic and antidepressant effects. Patient Experience: Highly rated and praised.
Result: High confidence for anxious depression (strong convergence across sources).
For Ruminative Depression: Clomipramine
When depression involves intense rumination or obsessional thinking.
Mechanism: Primary SERT blockade with active metabolite norclomipramine providing strong NET inhibition; additional 5‑HT2A/2C antagonism, sigma‑1 engagement, modest sodium‑channel effects, and antimuscarinic load. Net effect: heightened serotonergic tone with noradrenergic gating, dampening error‑signal propagation across cortico‑striato‑thalamo‑cortical (CSTC) loops. Predictions: ↓ intrusive/ruminative loops; improved cognitive gating; on fMRI, reduced hyperconnectivity in orbitofrontal–striatal circuits; behaviorally, ↓ checking/rumination latency and frequency on symptom‑provocation tasks. Trials: A wealth of data demonstrates its superiority over SSRIs for OCD, plus historical support for severe depression. Expert Opinion: Long-recognized as uniquely powerful for treatment-resistant obsessive presentations. Prescriber Observation: Causes significant breakthroughs in patients trapped in negative thought cycles. Patient Experience: Individuals describe a lifting of the mental burden, with reduced intrusive thoughts and unprecedented mental quiet.
Result: Very high confidence for ruminative depression (exceptionally strong convergence).
The Recognition
They wake into assembled mornings—
those who found their final pieces,
who learned which edges hunger for each other,
which fragments complete the picture
they were always meant to inhabit.
Remission wears their faces now.
Remember the corner pieces arriving,
how they promised architecture
beyond imagination?
Now they frame lives that hold:
these prophecies fulfilled,
these possibilities breathing
in kitchens, offices, embraces—
ordinary magic of the healed.
The measured ones that wouldn't fit
beyond their sterile borders
taught what completion isn't—
not perfect mathematical certainty,
but this wild, sustainable wholeness
that bends without breaking,
that knows bad days don't mean
the puzzle has scattered again.
Those heirloom pieces, worn smooth
by all who searched before,
finally reveal their secret:
they kept their faith because they'd seen
the completed pictures,
lived beside the friends who found
their last essential fragment
and stepped into wellness.
The field-tested pieces bear their scars
as proof—
not of damage, but of truth
earned through friction,
the beautiful specificity
of what actually works
for this person, this brain,
this irreplaceable configuration
of need and possibility.
Truth arrives when all languages
suddenly speak as one—
mechanism matching experience,
trials confirming intuition,
the prescription that becomes
the morning you wake up whole.
Not perfect. Not invulnerable.
But complete.
We witness daily transformations:
the one who tried seventeen medications
before the eighteenth clicked.
The one whose rare mutation
needed a forgotten drug.
The one who found their answer
in a combination no textbook suggests—
each teaching us: puzzles complete.
To those still searching:
your pieces exist.
We've seen too many find them
to believe otherwise.
They live full lives now,
send postcards from remission,
return to help others recognize
the patterns that lead home.
The recognition comes as certainty—
not that the search is easy,
but that completion is possible.
Someone solved this yesterday.
Someone will solve it tomorrow.
The frameworks evolve
because people keep finding their pictures,
proving what we thought impossible
is merely undiscovered.
Keep gathering. Keep trying.
Your constellation of symptoms has an answer.
Your suffering has a solution.
The picture you need exists—
vivid, breathing, complete—
waiting for the moment
when the last piece clicks
and you recognize yourself
in the landscape of the well.
Having explored the framework through metaphor and theory, we turn now to the practical wisdom gathered by our community. What follows are the patterns we've observed, the questions we hear most often, and the guidance that has helped others find their way. These insights emerge not from any single authority, but from the convergence of thousands of treatment journeys—each one teaching us something about what actually works. These practical insights underscore the central idea of convergence—grounding theory in lived realities.
Supporting Others: A Guide for Family and Friends
For anyone trying to help someone navigate severe mental health conditions.
If you've never experienced something like this before, there are things you need to understand. Try to imagine: Sometimes you cannot see yourself getting better. Every pattern you observe points toward darkness. Hope doesn't just diminish—it can be completely annihilated. The longer your intensive suffering continues, the more helpless you become. You may get angry and lash out at those you love. You may grow too sad to speak, too stuck to attempt any forward momentum. Why would you bother trying when nothing has worked? When you can't make it through the day, when pain eclipses every small joy, when there's no apparent reason to do much of anything: this is where you live.
The Art of Being There
Listen. That's where everything starts.
Try to understand what they're going through. And when you can't understand—when their experience is so foreign to your own that comprehension fails—you can still help by simply being there. If they want you there.
You might think presence is "all you can do," but presence is actually a hell of a lot. It is probably more than most people get.
What Actually Helps
Being Present:
Listen without judgment Acknowledge their experience as real Show up consistently when they want company Respect when they need space
Holding Both Truths:
Their pain is real AND it won't last forever This moment is unbearable AND moments change They can't see hope AND you can hold it for them Nothing has worked yet AND something eventually will
The Perspective Shift
They may not be able to see it, but you know the pain they're in won't last forever. Severe mental health conditions often feel permanent from the inside. From the outside, you can see what they cannot: that people get through this. That suffering, however intense, shifts and changes. That puzzles which seem impossible today become solvable tomorrow. Your job isn't to convince them. Your job is to know it for them until they can know it themselves.
When They're Stuck
People get stuck in patterns, in medications that half-work, in relationships with prescribers who've given up, and in the belief that this is just how they are. If they're open to it, you can help brainstorm ways to get unstuck. Sometimes a fresh perspective helps see options that feel invisible from inside the struggle.
But only if they want this help. Sometimes being stuck is all someone can manage, and pushing makes it worse.
Remember
Supporting someone through severe mental health struggles means different things on different days. Sometimes it's active help. Sometimes it's quiet presence. Sometimes it's holding space for pain. Sometimes it's holding hope they can't access. There's no perfect way to do this. But showing up, listening, and believing that things can change even when they can't matters more than you might realize.
Q&A
How do I know if my medication is working?
Step 1: Reach a therapeutic dose and maintain it for the recommended duration. Step 2: Assess the response: remission (stop), partial response (increase dose), or no response/intolerable side effects (switch). Step 3: If improved but not in remission, maintain the current dose and add a second medication. Step 4: Adjust the combination or switch the added medication based on the results.
Key Principles: A partial response is often worth building on rather than restarting. Long-term assessment matters more than the first few days. If you are unsure if it's helping after a year, it probably isn't.
How long does it take to respond to a medication?
Response time creates particular confusion for patients, and our multi-axial framework helps explain why. Different sources of evidence tell different stories: trials measure statistical response at specific timepoints, prescribers track functional improvement over months, experts recognize patterns across populations, and patients experience day-to-day changes. Each perspective captures part of the truth.
If you're starting a new medication, here's the essential principle that applies to most psychiatric medications: No matter how you respond in the first few days, your response will differ after taking the medication consistently for several weeks.
Understanding two broad response patterns helps set realistic expectations:
Stimulants and Sedatives:
Strongest effects begin within 30 minutes and peak within hours. This immediate response often resembles the therapeutic effect. Effects typically feel less powerful after weeks of repeated use.
Antidepressants:
Initial effects may appear within 72 hours. These early responses do NOT predict therapeutic benefit. Initial effects often diminish, while the therapeutic response emerges at 2-4 weeks. The antidepressant response is defined by sustained improvement over time.
When prescribers mention waiting "4-8 weeks," they're discussing the Antidepressant Response. While initial biological adjustments happen much faster, you are simultaneously developing new behavioral patterns in response to the medication. Biology and behavior intertwine in continuous loops: biological changes enable behavioral changes, which in turn reinforce biological changes.
Prescribers face a communication challenge. In limited appointment times, they must balance setting realistic long-term expectations, not overemphasizing initial side effects that often fade, and preparing patients appropriately without overwhelming them. This balancing act means prescribers often focus on the sustained response that matters most for recovery, rather than detailing every phase of adjustment.
How do I get my prescriber to prescribe a specific drug?
This is often the wrong question. A more productive one is: "How do I have a good conversation with my prescriber about whether [drug X] might help me?" This shift—from trying to get something to trying to explore something together—transforms the entire dynamic.
Remember that you and your prescriber each hold different pieces of the same puzzle.
What Prescribers Bring: Years of medical education and pattern recognition, clinical experience with thousands of patients, understanding of drug interactions and medical complexity, and the responsibility to not cause harm.
What Patients Bring: Direct experience of symptoms from the inside, knowledge of what daily life with the condition actually entails, memory of how previous medications felt (not just how they "worked"), and an understanding of their own values and acceptable trade-offs.
No amount of medical training grants access to another person's inner experience. When you say, "SSRIs make me feel emotionally blunted," you're reporting qualia that no rating scale can fully capture.
What can help with anhedonia?
This seemingly simple question reveals profound complexity. Consider the challenges: What if anhedonia's causes vary dramatically between individuals? What if drugs targeting reward systems work only temporarily, unless paired with behavioral changes that foster long-term engagement? What if the quicker a drug shows results, the less sustainable those effects prove?
Stimulants can provide temporary engagement—increased focus and motivation. But patients often remain intensely aware these effects will wear off, leaving the underlying depression untouched. They create a dramatic change of feeling very quickly, and tolerance forms just as fast.
Rather than seeking simple answers, consider these questions (they're designed to stimulate insight, not to be answered here):
Are you maintaining basic health practices: eating, hydrating, exercising, sleeping, connecting with others? What's your family history of mental health conditions? How did your mental health issues develop over time? How does anhedonia affect you throughout a typical day, and what patterns do you notice? What has been your experience with previous medications? Are you using substances that might worsen your condition? Do you have any physical health issues or recent major life stressors? How do you typically cope with difficult emotions? Do you have meaningful goals or purpose? What are you hoping medication will accomplish?
These questions illustrate how a single symptom can emerge from multiple pathways, requiring different approaches—a perfect example of why the multi-axial framework is necessary.
How do I get more dopamine?
You probably don't need "more dopamine." Pharmacological dopamine increases affect mood, attention, drive, risk-taking, impulsivity, and sleep. It is better to target symptoms, not neurotransmitters.
How do I reset tolerance?
There is no reliable method besides medication holidays, which carry risks and require medical supervision. Some people regain sensitivity over time, but no guaranteed shortcuts exist.
Is cannabis safe?
It won't kill you, but its use negatively correlates with outcomes in nearly every mental disorder, especially with regular use. It is not evil, but it is not neutral. It tends to worsen depression, anxiety, and psychosis.
What about therapy?
Many who could benefit from it are not using it. Therapy plus medication is usually the most effective approach if it is affordable in terms of time and cost. Treat therapy like medication: try it, give it time, and switch if it is not helping.
Who doesn't get better?
Most people do. Three patterns are common in those who stay stuck:
Ongoing recreational drug use: The body can't stabilize enough for recovery. Rigidity: An inability to adapt strategies (if you're reading this, this is probably not you). Isolation: A lack of support. Even one person reminding you "this is temporary" can save your life.
Appendix A: Quick Reference - The Five-Axis Framework
EVIDENCE
SHOWS
RED FLAG
Mechanism
How it should work
"It has to work because..."
Trials
Statistical efficacy
"Studies prove..." (in artificial conditions)
Experts
Pattern recognition
"We've always done this..."
Prescriber
Real-world use
"All my patients..." (selection bias)
Patients
Lived outcomes
"I feel better" (while worsening)
Truth emerges when all five converge. Suspect single sources that claim complete knowledge.
Appendix B: A Brief Guide to Reading Research Papers
Why Read Primary Sources?
Understand what studies actually showed Evaluate applicability to your situation Ask better questions of your provider Contribute meaningfully to discussions
Where to Find Papers
Free: PubMed Central, Google Scholar, ResearchGate, emailing authors Libraries: Public, university alumni, advocacy organizations
Paper Anatomy
Abstract: A 250-word summary to decide relevance. Introduction: Background to understand the rationale. Methods: How it was conducted to assess quality. Results: What was found to see the actual outcomes. Discussion: Interpretation to understand the implications. Limitations: Study weaknesses for crucial context.
Red Flags
Exclusion of complex patients Very short duration High dropout rates Focus on statistical vs. clinical significance Industry funding without transparency
Statistics Basics
p-value: Likelihood of chance (not importance). Effect size: The magnitude of the actual difference. NNT: Number needed to treat for one person to benefit. Confidence intervals: The range of likely true effects.
Making Sense of Contradictions
It is normal to find opposing studies. Consider different populations, doses, durations, outcome measures, publication bias, and study quality.
Applying to Your Situation
You are not a statistical average. Studies show probability, not certainty. Research informs decisions but doesn't make them. Your lived experience is also data.
Good Starting Points
Review articles: Systematic reviews and meta-analyses (though these can be very introductory as they often compound problems from the original studies), Cochrane reviews. Clinical guidelines: Starting points, not rules. Patient-centered research: PCORI, studies including patient perspectives.
Papers are puzzle pieces, not complete pictures. Their best use is to inform discussions with providers, understand trade-offs, and recognize when your situation differs from studied populations.
Appendix C: Thinking Critically: A Guide to Scientific Skepticism in Psychiatric Medicine
When the pieces don't fit the way they're supposed to.
In our search for therapeutic truth, we encounter not just puzzle pieces, but people insisting they know exactly how those pieces should fit. This chapter offers tools for maintaining healthy skepticism while remaining open to genuine discovery.
Red Flag Phrases in Medical Discourse
When evaluating claims about psychiatric treatment, certain phrases should trigger deeper investigation:
"The science is settled": Science is never settled—it evolves. What we "knew" about serotonin's role in depression has shifted dramatically over decades. Settled science once included lobotomies and insulin comas.
"I believe the science": Which science? Whose interpretation? Science isn't a monolith requiring faith—it's a method requiring examination.
"It is a scientific fact": Science deals in observations, replications, and probabilities—not immutable facts. Even our most reliable findings carry uncertainty.
"The experts agree": Which experts? Funded by whom? Speaking from what perspective? Remember: experts once agreed that MAOIs were too dangerous for routine use, missing their unique efficacy for specific patients.
"That has been thoroughly debunked": Has it? Or has it been dismissed without proper examination? Many effective treatments were "debunked" before being vindicated. Re-examine the evidence yourself.
"It's just a conspiracy theory": Sometimes fringe ideas contain kernels of truth. The psychiatric establishment's resistance to patient-reported SSRI withdrawal was dismissed as conspiracy thinking—until the evidence became undeniable.
Reading Research with Clear Eyes
When examining studies, always ask:
Why does this paper exist? What prompted this research? Is it addressing genuine clinical questions or serving other interests? Who funded this study? Follow the money. Industry-funded trials showing positive results for patented drugs deserve extra scrutiny. What's the agenda? Everyone has one—researchers, journals, your prescriber, even you. Recognizing agendas helps evaluate information more clearly.
Critical Thinking Principles
Theory ≠ Practice: Beautiful receptor binding studies don't guarantee real-world efficacy. What works in test tubes may fail in humans. The gap between mechanism and experience is where many treatments falter.
Correlation ≠ Causation: Depression correlates with inflammation, but which causes which? Maybe both stem from a third factor. This matters when choosing a treatment.
Publication Bias is Real:
Positive results get published; negative results get buried. Industry-funded studies showing unfavorable results often disappear. Meta-analyses can compound these biases. When you see uniform positive results, be suspicious.
The Coherence Test
When evaluating any claim about psychiatric treatment, apply the coherence test:
Single-source claims are suspect: "Studies prove..." or "Patients say..." or "The mechanism shows..." should trigger skepticism. Truth in psychiatry rarely comes from one direction.
Look for convergence patterns: Does the biological story match the behavioral story? Do experts recognize what patients report? Does real-world practice align with controlled trials?
Investigate divergence: When sources disagree, that's information too. Why might trials show efficacy while patients report failure? Why might mechanism predict one thing while experience shows another? These gaps often reveal hidden variables.
Weighted coherence: Not all convergence is equal. Five pharmaceutical company studies agreeing carries less weight than independent evidence from different types of sources agreeing.
Remember: We're not choosing which authority to believe. We're mapping how different types of evidence relate to each other. The map, not any single landmark, guides us toward therapeutic truth.
Your Puzzle, Your Truth
Remember: you might be onto something others can't see. Maybe you've noticed patterns your prescriber dismisses, benefits at "wrong" doses, side effects no one talks about, or a medication that works differently than studies suggest.
Some will discourage your observations with good intentions or bad. Some can't see what you see. Some don't want others to see it. Hold onto your insights while remaining open to correction.
Remember: Every breakthrough began with someone noticing what others missed.
About the Psychopharmacology Community
Our Discord server uniquely combines rigorous scientific discussion with genuine human support. Founded on the principles that we can study medication, help people, and build meaningful friendships simultaneously, the community has grown into a vital resource for those navigating psychiatric treatment.
Our Mission:
Explore medication intricacies: Delving deep into the mysteries of psychopharmacology. Commit to support: Offering unwavering assistance to make a meaningful difference. Cherish friendship bonds: Fostering a warm environment where camaraderie flourishes.
Questions are welcomed, experiences flow freely, and no one navigates their journey alone. Whether trying the first medication or the fifteenth, whether in remission or still searching, members find both scientific insight and human understanding.
The server represents epistemology in action—where theoretical knowledge meets practical experience, individual stories combine to reveal patterns, and the understanding of psychiatric medication happens collaboratively.
Join the conversation: Discord.gg/NwvxKxUJpC
"At our community's heart, we explore, support, and connect."